


























Success
Management of urinary tract infections in the era of antimicrobial resistance: An update
Nov 10, 2021
Explore More

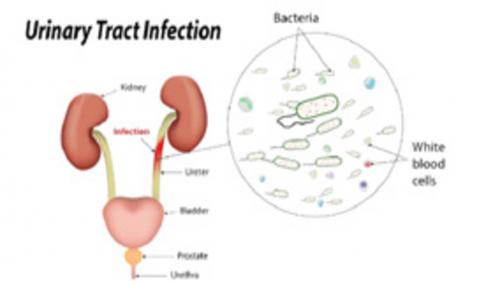
A growing concern is urinary tract infections (UTIs) that are caused by antibiotic-resistant Gram-negative bacteria due to limited therapeutic options. Gram-negative bacteria, specifically Enterobacteriaceae, are common causes of both community-acquired and hospital acquired UTIs. These organisms can attain genes that encode for multiple antibiotic resistance mechanisms, including extended-spectrum-lactamases (ESBLs), AmpC- β -lactamase, and carbapenemases. The evaluation of suspected UTI includes identification of characteristic symptoms or signs, urinalysis, dipstick or microscopic tests, and urine culture if indicated.
UTIs are categorized according to severity (uncomplicated versus complicated) and location (upper versus lower urinary tract). Since antibiotic resistance rates are increasing, judicious use of antibiotics has become a necessary step through the application of antimicrobial stewardship principles. Knowledge of the common causative pathogens of UTIs including local susceptibility patterns is vital in the decision of an appropriate empiric therapy.
- Recommended first-line empiric therapies for acute uncomplicated bacterial cystitis in otherwise healthy adult nonpregnant females are a 5-day course of nitrofurantion or a 3-g single dose of fosfomycin tromethamine
- Second-line options: Fluoroquinolones and β-lactams, such as amoxicillin-clavulanate
- Current treatment options for UTIs due to AmpC- β -lactamase-producing organisms: Fosfomycin, nitrofurantion, fluoroquinolones, cefepime, piperacillin-tazobactam and carbapenems
- Treatment options due to ESBLs-producing Enterobacteriaceae: Nitrofurantion, fosfomycin, fluoroquinolones, cefoxitin, piperacillin-tazobactam, carbapenems, ceftazidime-avibactam, ceftolozane-tazobactam, and aminoglycosides
- Based on identification and susceptibility results, alternatives to carbapenems may be used to treat mild-moderate UTIs caused by ESBL-producing Enterobacteriaceae
- Treatment options for UTIs caused by carbapenem-resistant Enterobacteriaceae (CRE): Ceftazidime-avibactam, colistin, polymixin B, fosfomycin, aztreonam, aminoglycosides, and tigecycline
- Treatment options for UTIs caused by multidrug resistant (MDR): Pseudomonas spp. include fluoroquinolones, ceftazidime, cefepime, piperacillin-tazobactam, carbapenems, aminoglycosides, colistin, ceftazidime-avibactam, and ceftolozane-tazobactam
- Use of fluoroquinolones for empiric treatment of UTIs should be restricted due to increased rates of resistance
- Aminoglycosides, colistin, and tigecycline are considered alternatives in the setting of MDR Gram-negative infections in patients with limited therapeutic options
Reference: Bader MS, et al. An update on the management of urinary tract infections in the era of antimicrobial resistance. Postgrad Med. 2016 Oct 7.